
From the 1Department of Physical Medicine & Rehabilitation, Chonbuk National University Medical School, 2Research Institute of Clinical Medicine of Chonbuk National University-Biomedical Research Institute of Chonbuk National University Hospital, 3Translational Research & Clinical Trial Center for Medical Device, Chonbuk National University Hospital, Jeonbuk, Republic of Korea
Objective: Robot-assisted rehabilitation therapy of the upper extremity after stroke has been studied widely; however, robotic devices remain expensive and bulky. The aim of this study was to evaluate the effects of a newly developed, compact upper extremity training system (Neuro-X®) in patients with chronic stroke.
Design: Pilot study.
Subjects: Fifteen patients with hemiplegia.
Methods: Chronic patients with stroke underwent upper extremity training using a newly developed upper extremity training system (Neuro-X®; Apsun Inc., Seoul, Korea). Patients were evaluated using the Fugl-Meyer Assessment (FMA), Hand Function Test (HFT), Modified Ashworth Scale (MAS), and Korean Mini-Mental Status Evaluation (K-MMSE). The assessment started with “pre 1 evaluation” (A1), followed by repeated “pre 2 evaluation” (A2) after 6 weeks without receiving any treatment, in order to generate repeated baseline data. After the A2 evaluation, upper extremity training was performed for 6 weeks. Post-training evaluation (B) was performed after treatment. Obtained data (A1–A2–B) were compared.
Results: During the non-intervention phase (A1 to A2), no significant changes were found in the aforementioned evaluations. However, in the intervention phase (A2 to B), results of the FMA and HFT, and K-MMSE scores, except the MAS score, increased significantly (p < 0.05).
Conclusion: The Neuro-X® training system improves functioning of the upper extremity and cognition in patients with stroke after 6 weeks of training.
Key words: robotics; rehabilitation; stroke; upper extremity.
Accepted April 25, 2018; Epub ahead of print Jun 26, 2018
J Rehabil Med 2018; 50: 598–603
Correspondence address: Myoung-Hwan Ko, Department of Physical Medicine & Rehabilitation, Chonbuk National University Medical School and Hospital, 20, Geonjiro, Deokjin-gu, Jeonju City, 561-712, Jeonbuk, Republic of Korea. E-mail: mhko@jbnu.ac.kr
Although robot-assisted rehabilitation therapy of the upper extremity after stroke has been widely studied, robotic devices are still expensive and voluminous. This newly developed compact upper extremity training system (Neuro-X®) was inexpensive, small-sized, easy to move, and has two muscle strength measurements and six treatment modes. We aimed to evaluate the effects of newly developed compact Neuro-X® system in patients with chronic stroke. Neuro-X® training system can improve the function of the upper extremity and cognition in patients with stroke after six weeks of training and be used for functional recovery of the upper extremity in patients with stroke.
Persistent impairment of upper extremity motor functioning is common after stroke and involves the motor area of the brain. Although weakness of the upper extremity might not be severe, the paretic arm in patients with hemiplegia could limit activities of daily living and contribute to stroke-related disability (1–4). In general, reduced upper extremity functioning has been reported even in stroke survivors who have made a good recovery.
Various attempts have been made to improve motor functioning of the affected upper extremity in patients with hemiplegia. Repetitive movement training, based on the neuroplasticity of the affected side of the brain after stroke, has been reported to contribute to functional recovery of hemiplegia. In this context, high-intensity repetitive training for functional recovery of the upper extremity has been used in rehabilitation (4–7). Among the devices and methods for high-intensity repetitive training of the affected extremity, robotic systems have been found effective for improving motor recovery of patients with stroke over recent decades (8–11). In addition, a robotic system for upper extremity rehabilitation can safely improve upper extremity functioning in patients with subacute and chronic stroke (12, 13). Robot-assisted upper extremity training has been reported to be an effective treatment based on brain neuroplasticity studies, and the clinical application of robotic-aided therapy has been increasing (8, 14–16).
However, these robotic devices are still expensive and are too bulky to be used in a therapy room. The newly developed, compact Neuro-X® system (Apsun Inc., Seoul, Korea) was designed to be small (width × depth × height 580 × 1,100 × 1,250 mm, weight 75 kg), inexpensive (USD 24,000), and easy to move. The system allows various muscle strength measurements and different therapeutic game modes. The aim of this study was to evaluate the effects of rehabilitation treatment after 6 weeks of upper extremity training in patients with hemiplegia caused by stroke using this newly developed, compact robot device (Neuro-X®).
The present study included chronic stroke patients with hemiplegia, who were followed up as outpatients at the Department of Rehabilitation Medicine of Chonbuk University Hospital between March 2014 and November 2015.
The inclusion criteria were: (i) first stroke caused by cerebral haemorrhage or infarction, occurring more than 6 months before study inclusion; (ii) age between 20 and 85 years; (iii) Fugl-Meyer upper motor scores (FMA-UE) over 18; and (iv) voluntary agreement and provision of signed consent form. Exclusion criteria were: (i) patients with severe cognitive impairment or aphasia who could not follow the examiner’s instructions and with Korean Mini-Mental Status Evaluation (K-MMSE) scores below 18; (ii) current severe medical diseases; and (iii) patients deemed unsuitable by the examiner for participation in the clinical study for other reasons.
Ethical approval for the study was obtained from our institutional review board (IRB) (IRB number 2013-08-020).
This study had an exploratory design with a baseline phase (A1), intervention phase (A2), and post-test phase (B). The study began with the pre-1 evaluation (A1) followed by the pre-2 evaluation (A2) (after 6 weeks with no treatment), which repeated the pre-1 evaluation to generate the repeated baseline data. After these 2 pre-evaluations, subjects performed upper extremity training with the Neuro-X® for 6 weeks. Subsequently, post-training evaluation was performed immediately after treatment (B). Data obtained during each evaluation (A1–A2–B) were compared.
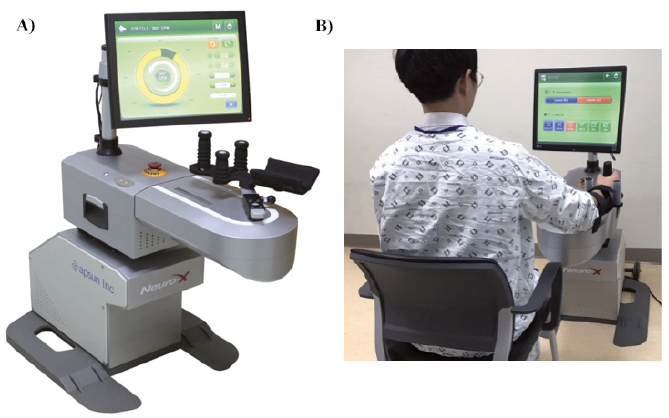
During the robot-assisted upper extremity rehabilitation treatment with the newly developed robot-aided upper extremity training system (Neuro-X®) (Fig. 1A), subjects were seated comfortably in a chair in front of the robot. The hemiplegic upper extremity was attached to an arm support located at the end of the device (Fig. 1B). The patients’ trunk was restricted by the therapist to decrease compensatory motions. Patients received 40 min of robotic therapy 3 times per week for 6 weeks, which included repetitive reaching tasks provided on the screen by the Neuro-X® system (Fig. 2A–C).
Fig. 1. (A) The newly developed upper extremity training system (Neuro-X®; Apsun Inc., Seoul, Korea) consists of a game monitor and an upper limb exercise plate. (B) Subjects were seated comfortably in a chair in front of the robot. The hemiplegic upper extremity was attached to the arm support located at the end of the device.
Fig. 2. Three modes of the training program in the Neuro-X® system (Apsun Inc., Seoul, Korea). (A) The isometric task-specific program, goalkeeper game, is programmed to randomly block a ball randomly on the left and right sides of the monitor. (B) The 360° range of motion (ROM) active-assisted program, gliding mill-stone games, enhances shoulder and elbow joints’ ROM by repetitive 360° ROM exercise with constant resistance according to the individual’s potential. (C) The ROM active-assisted program, the dolphin circus game, is a mode in which the patient actively moves his or her arm within the set ROM. The patient must produce force above the threshold (green part of the bar on the left of the screen) to allow the program to proceed or to perform the task. All the game programs prompted the participants’ concentration through sound effects. The scores at the top left are the target score as the numerator, and the success score as the denominator.
The Neuro-X®, a rehabilitation treatment system created for the hemiplegia-affected upper extremity, has been developed for correct motion, active, and repetitive exercise, and task-specific exercise. The planar robotic arm was attached to the robot and designated to perform 2° forearm movements (shoulder abduction-adduction and elbow flexion-extension movements in the horizontal plane).
This device has 2 muscle strength measurements and 6 treatment modes. The muscle strength measurement programs consisted of isometric and isokinetic measurements, and the treatment mode was designed as a game in the isometric task-specific mode, range of motion (ROM) assist active motion (AAM) mode, 360° AAM mode, ROM continuous passive motion mode, non-resistant task-specific mode (task refers to activities of daily living), and active passive motion mode. In this study, the isometric task-specific mode, ROM AAM mode, and 360-degree AAM modes were used. The treatment comprised active-assisted games, which could be performed by patients, and provided visual feedback to help goal-oriented tasks that were performed according to the goal or target provided to the patient during training. The method of muscle strength measurement was adjusted for each treatment mode at the beginning of treatment.
Various ROMs of the robotic arm were conveyed as a single signal through a robot’s sensor, which allowed sensing of the patient’s movements and measurement of patient’s strength. Therefore, subjects’ motor threshold values were assessed through isometric and isokinetic measurements in the initial stage of the robot program, and movements were enabled by the patient’s remaining strength. After assessing the movements obtained at the early stage of each treatment session to determine proper exercise intensity, threshold values of muscle strength were entered in a database. The game could be played only when the measured strength was higher than the previous setting threshold
Patients were evaluated using the Fugl-Meyer Assessment (FMA), Manual Muscle Test, Hand Function Tests (HFTs), Modified Ashworth Scale (MAS), and Mini-Mental State Evaluation (MMSE). These tests were first conducted during the A1 phase, and all evaluations were subsequently repeated during the B phase. Post-training evaluations (A2) were performed after 6 weeks of upper extremity training.
The FMA is a widely used scale to assess motor impairment in patients with stroke. The FMA-UE was used to evaluate the function of the affected upper extremity (17, 18). According to previous studies on robotic rehabilitation, this scale is commonly used to assess motor improvement. The scale consists of 62 items. Among the 62 items, the FMA-UE shoulder/elbow and coordination (SEC) subsection (FM–SEC = 42/66), wrist/hand (WH) subsection (FM–WH = 24/66), and total score (FMA-UE = 66) were used in this study because the Neuro-X® could be used to treat only the upper extremity (19, 20).
HFTs included the Grip Strength Test, Box and Block Test, and 9-Hole Peg Test (NHPT). These tests were used to assess the strength and dexterity of the affected hand (21). For grip strength, the hand dynamometer (JAMAR®, Chicago, IL, USA) was used to measure the maximum grip power. The Box and Block Test was used to assess gross manual dexterity by counting the number of blocks moved from one box to the other for 1 min. The NHPT was used to assess fine manual dexterity by measuring the time it took each patient to place 9 pegs one at a time into 9 holes and then to remove them one at a time.
The MAS (range 0–4) were used to assess spasticity of the affected extremity (22).
The neurocognitive function test used in the present study was the K-MMSE (23).
Statistical analyses were performed using SPSS, version 24.0 statistical software (SPSS Inc., Chicago, IL, USA). For data obtained in each phase (A1-A2-B), the values of the examinations are presented as mean values and standard deviations (SD), and ordinary scales are described as medians and interquartile ranges (IQR). Comparisons between the differences in the non-intervention phase (A1 to A2) and differences in the intervention phase (A2 to B) were computed and statistically compared using the paired t-test for normally distributed variables (Box and Block Test, and MAS), whereas the Wilcoxon signed-rank test was used for other tests that showed non-normally distributed variables. The p-value < 0.05 was considered statistically significant.
During the study period, 20 hemiplegic patients with stroke visited our department. Of these, 5 were excluded from the study because they did not satisfy the enrollment criteria, and 15 patients were consecutively enrolled in the study. One patient dropped out because of personal reasons. Fourteen patients completed the training programme with the Neuro-X® (11 men and 3 women, mean age 57.64 years (SD 2.21)). Six patients had right hemiplegia and 8 had left hemiplegia. The cause of the condition was ischaemic stroke in 11 patients and haemorrhagic stroke in 3 patients. The mean duration of illness was 44.07 months (SD 4.25).
No major or minor adverse effects were found during the training programme. During the non-intervention phase (A1 to A2), no significant changes were noted in the scores of hand function, FMA, MAS, and K-MMSE (p > 0.05, Tables I and II). However, after the training, the mean Hand Grip Strength, Box and Block Test, and NHPT scores significantly improved from 6.14 (SD 6.63) to 7.29 (SD 7.75) (p = 0.017), from 10.50 (SD 9.39) to 15.07 (SD 13.79) (p = 0.008), and from 14.50 s (SD 20.92) to 12.71 s (SD 18.45) (p = 0.043), respectively (Table I). The total FMA-UE score improved significantly from 30.71±12.96 to 33.64 (SD 15.25) (p = 0.001), and the proximal and distal sub-scores improved significantly from 23.36 (SD 6.71) to 25.50 (SD 8.00) (p = 0.001) and from 7.50 (SD 7.11) to 8.14 (SD 7.82) (p = 0.041), respectively. Moreover, the K-MMSE score improved from 27.36 (SD 2.76) to 28.50 (SD 2.10) (p = 0.013) after Neuro-X® training. The MAS score changed from 2.07 (SD 0.92) to 2.00 (SD 0.88), but the change was not statistically significant (p = 0.317) (Table II).
Table I. Comparison of affected upper extremity hand function test scores after training
Table II. Comparison of affected upper extremity function test scores, spasticity and cognitive function after training
This pilot study evaluated the movements that could be performed by residual upper extremity muscle strength in patients with hemiplegia caused by stroke, and revealed that intensive treatment using the newly developed robot-assisted upper extremity training system Neuro-X® for 6 weeks could improve the function of the patient’s affected upper extremity and cognitive function.
Various extremity rehabilitation treatments are available for patients with stroke, such as conventional rehabilitation therapy, constraint-induced movement therapy (CIMT), functional electrical stimulation, orthoses, and robot therapy (15). CIMT has a limitation of being only applicable to patients who have a certain degree of voluntary movement in the affected upper extremity (24). Moreover, it is difficult for a therapist to treat numerous patients or help them exercise with consistent intensity daily using previous conventional rehabilitation therapy, since one therapist can treat only one patient at a time in Korea and the work intensity of the therapist is high. Furthermore, it is difficult to obtain quantitative physiological information of patients during the exercise (25). As an alternative to overcome the limitations of previously mentioned treatments provided to patients with stroke, the upper extremity rehabilitation treatments using robots have been introduced, and their positive effects have been reported recently (15, 16). However, these robotic devices are still expensive and take up too much space in the therapy room.
This study evaluated the effect of rehabilitation treatment using the newly developed, compact upper extremity training system Neuro-X® in patients with chronic stroke. In this context, the characteristics of the Neuro-X® training system used in this study can be summarized as follows. First, the Neuro-X® is inexpensive (USD 24,000), small in size (width × depth × height 580 × 1,100 × 1,250 mm, weight 75 kg), and easy to move. Therefore, it will increase the clinical use of robotic-aided upper extremity rehabilitation, and make it more convenient and usable for patients. Secondly, patient’s motor threshold values were assessed through isometric and isokinetic measurements before the beginning of the exercise. After assessing threshold values, the training could be conducted only when the muscle strength exceeded the previous threshold. Furthermore, the threshold values gradually increased according to the individual’s characteristics and levels of improvement; therefore, the intensity of training could be naturally altered. These force feedbacks with a constant intensity for movements of the affected arm can be consistently provided during the training. Thirdly, the Neuro-X® has various treatment modes. The task-specific mode is training for moving the arm exactly on the target or giving the direction of the force. The CPM mode is a passive exercise mode that automatically moves within a certain range if the desired angle or speed is set. When the patient’s strength is measured during exercise, it is possible to switch to APM or AAM mode. The APM mode is a passive exercise mode in which the handle is moved automatically by the force of the robot. When the patient’s movement is detected, the mode is switched to active. When the patient’s movement is lost, the mode is switched to the passive exercise mode. The AAM mode does not provide assistance with the movement of the arm if the patient does not intend to move, but if the patient is willing to move, it detects it and begins movement. Because Neuro-X® has many exercise modes it can be widely used in various patients. Finally, visual games in robotic devices replaced the exercises that could be performed and had positive effects because they stimulated patient’s internal competitive spirit, and improved treatment compliance and satisfaction. The game programs improved interest and pleasure during treatment, thereby facilitating motor learning and recovery (15, 26–28). In our study, the treatment response of the patients was similar to the results of previous studies.
The functional evaluations after Neuro-X®-aided upper extremity training in this study showed improvement as in previous studies using upper extremity rehabilitation robots in patients with stroke (29–31). The functional recovery mechanism of the upper extremity induced by the Neuro-X® used in this study is likely to be associated with motor learning, motor adaptation, and compensation among various recovery mechanisms of the brain (32, 33). In general, recovery of the brain function is known to be achieved by repeated exercise training with high intensity. Therefore, the recovery mechanism after brain damage can be viewed as a process induced by exercise training. Previous studies have reported that higher intensity and active-assisted mode of the robot-assisted therapy movement may lead to better improvement in motor function (30, 34, 35). Upper extremity training in patients with stroke using the Neuro-X® provides an environment that allows suitable training of each patient using the maximum remaining muscle strength of the affected arm. In addition, because the equipment was designed to allow task-specific repetitive training, it is a reliable robot-assisted rehabilitation treatment.
The intervention phase (A2 to B) also significantly increased the K-MMSE scores that indicate cognitive function. The mechanisms that contribute to improvement in cognitive functioning are not fully understood. Cognitive and physical functions are known to be closely related (36). The robot that aided upper extremity training in patients with stroke has been shown to elicit motor learning and adaption. Improved cognitive function is thought to be a motor learning and adaptation process that results from numerous movement repetitions during the training period.
The MAS score for muscle spasticity showed a slight decrease after robotic therapy, but the difference was not significant. This result is in line with those of previous studies (37, 38).
This study has several limitations. First, the robotic training system for the upper extremity used in this study was not compared with conventional rehabilitation therapy or with other robotic groups. Therefore, we cannot confirm that it is as effective as conventional rehabilitation therapy. In addition, the number of study subjects was small, and the study did not have a cross-over design and lacked a repeated control several weeks after the end of the intervention. Finally, subjects were not homogeneous. Although patients in the acute phase of stroke were excluded, the duration of illness varied from the subacute to the chronic phases, and patients with a wide age range were included. More studies on upper extremity training using Neuro-X® should be performed in a larger group of patients with stroke, and this treatment should be compared with conventional rehabilitation therapy or other robotic device groups.
Robot-assisted upper extremity rehabilitation treat-ment using the compact Neuro-X® for 6 weeks in patients with hemiplegia caused by stroke may improve upper extremity functions. The compact Neuro-X® may increase the clinical use of robot-assisted upper extremity rehabilitation because of its effectiveness, low cost, small size, and easy handling.
This research was supported by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number: HI15C1529).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize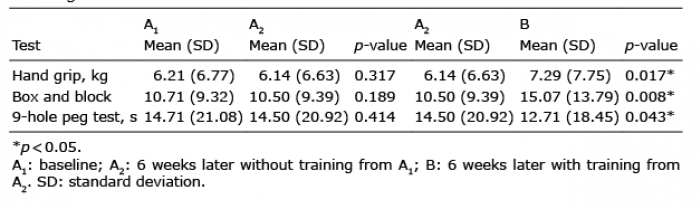 Click to show fullsize
Click to show fullsize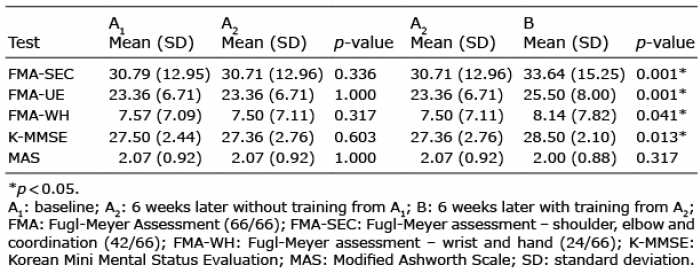 Click to show fullsize
Click to show fullsize